
•135 patients with liver cirrhosis.
•FibroTouch was applied to detect the liver stiffness measurement (LSM), and FIB-4 index was calculated.
•The differences in LSM and FIB-4 index among patients with different Child-Pugh classifications, patients with compensated or decompensated cirrhosis and patients with single complications or multiple complications were analyzed.
•Logistic analysis was used to predict the risk for occurrence of complications, and ROC curves were used to evaluate its predictive value.
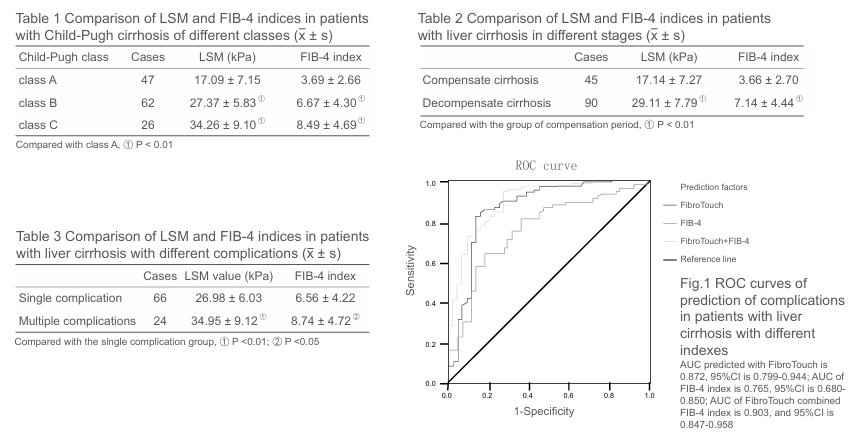
•The LSM in patients with Child-Pugh class A was (17.09 ± 7.15) kPa, significantly lower than that in with Child Pugh class B [(27.37 ± 5.83) kPa, P < 0.01] or that in with Child-Pugh class C [(34.26 ± 9.10) kPa, P < 0.01]; the FIB-4 index in patients with Child-Pugh class A was (3.69 ± 2.66), significantly lower than that in with Child-Pugh class B[(6.67 ± 4.30), P < 0.01] or that in with Child-Pugh class C [(8.49 ± 4.69), P < 0.01] The LSM in compensated cirrhosis patients was (17.14 ± 7.27) kPa, significantly lower than that in the decompensated cirrhosis patients [(29.11 ± 7.79) kPa, P < 0.01].
•The FIB-4 index in compensated cirrhosis patients was (3.66 ± 2.70), significantly lower than that in the decompensated cirrhosis patients [(7.14 ± 4.44), P < 0.01].
•The LSM in patients with single complication was (26.98 ± 6.03) kPa, significantly lower than that in with multiple complications [(34.95 ± 9.12) kPa, P < 0.01].
•FIB-4 index in single complication patients was (6.56 ± 4.22), significantly lower than that in multiple complications patients [(8.74 ± 4.72), P < 0.01].
•The AUC of FibroTouch combined with FIB-4 index to predict complications in patients with liver cirrhosis was 0.903, significantly higher than that by FIB-4 index alone (0.765, P < 0.01).